Recently, I wrote a post on recruitment in a tough labor market. Suffice to say, I have not in my three decades plus career, seen a tougher labor market for clinical staff (all staff in many regards). COVID had a lot to do with the shifting supply of labor, but I’ll offer that health policies and economic policies during the prime pandemic period and since, had far more to do with where staff went – and clearly, stayed. Societal and government responses to COVID are in my opinion, primarily to blame for the largest impact on staff disengagement from direct care environments. Dissecting the policy side is a topic for another post on another day. The recruitment strategy post can be found here: https://wp.me/ptUlY-vj
The opposite of recruitment is retention. Arguably, the better an organization does at retaining its employees, the less it needs to invest in recruitment. Healthcare has notoriously been an industry prone to turnover, especially among para and non-professional staff. Back in the day (I sound like a codger), I knew some long-term CNAs, ten to even thirty years in one company (one I was running at the time) and similar for housekeepers, laundry staff and maintenance. I simply don’t see that kind of tenure any longer, save a few of the folk almost at retirement. Once the final generational shift occurs, primarily the folk in my age cohort (aka “Boomers”), new outlooks on longevity in one career and one employer become fully operable. Simply, length of service regardless of retention strategy will be shorter. Long-term may evolve to any service in one place between 5 to 10 years. Outliers will be those working in the same place for ten plus years, without a shift in position or level within the organization (e.g., move to management or some other promotion).
Combatting turnover is a function of understanding why people leave, voluntarily. Some of the primary conditions are symptoms of what is going on in the healthcare industry. For example, hours and workload are often cited as primary drivers yet, providers have (often) little choice but to mandate overtime or have folks work short, covering more patients (or cases) than ideal. There is a bit of a circular (dog chasing his/her tail) phenomenon about workload when overall, open positions exist. Staff get tired of working short or covering for call-offs, etc., and thus, turn over. Problem is perpetuated. A somewhat universal list of the top reasons staff leave is below.
- Supervision: Bad managers/supervisors create turnover.
- Recognition: This is different from reward. This is appreciation or acknowledgement of the work being done within the conditions/environment that it is being done in.
- Schedule/Workload: This involves everything from how much patients/cases are on the shift to when shifts change or rotate to length of shifts to weekends to on-call to overtime mandates, etc. Extra hours can sometimes be absorbed without too much difficulty but too often as of late, extra hours are the norm and staff burnout.
- Limited Promotion/Growth: Healthcare is very layered and often, the jobs stagnate. For example, lateral movement is difficult at a professional level. RNs in one area can’t always jump to another clinical area without additional training or without taking a back-step in schedules, etc. If the view is that the only promotion is to management, a couple of realities need to be considered. First, not all (or even most) clinical staff make good management/supervisory staff. The industry definitely does not need more weak managers. Second, taking good clinicians away from patient care is self-defeating to the organization and to the patient.
- Bureaucracy/Regulation: This I’ll call paper before patients. Healthcare as I often hear, is neither fun nor rewarding in the way it used to be. Too much regulation takes the clinicians who went into the industry away from patient relationships. Staff have tons of work to do and on top, supervisors crab constantly about keeping paperwork up to date (documentation). Meetings and in-services are constant and rarely, of any value (per staff). Don’t forget too, the industry lost untold numbers due to COVID mandates (vaccine, PPE, testing) that created massive burnout and frustration.
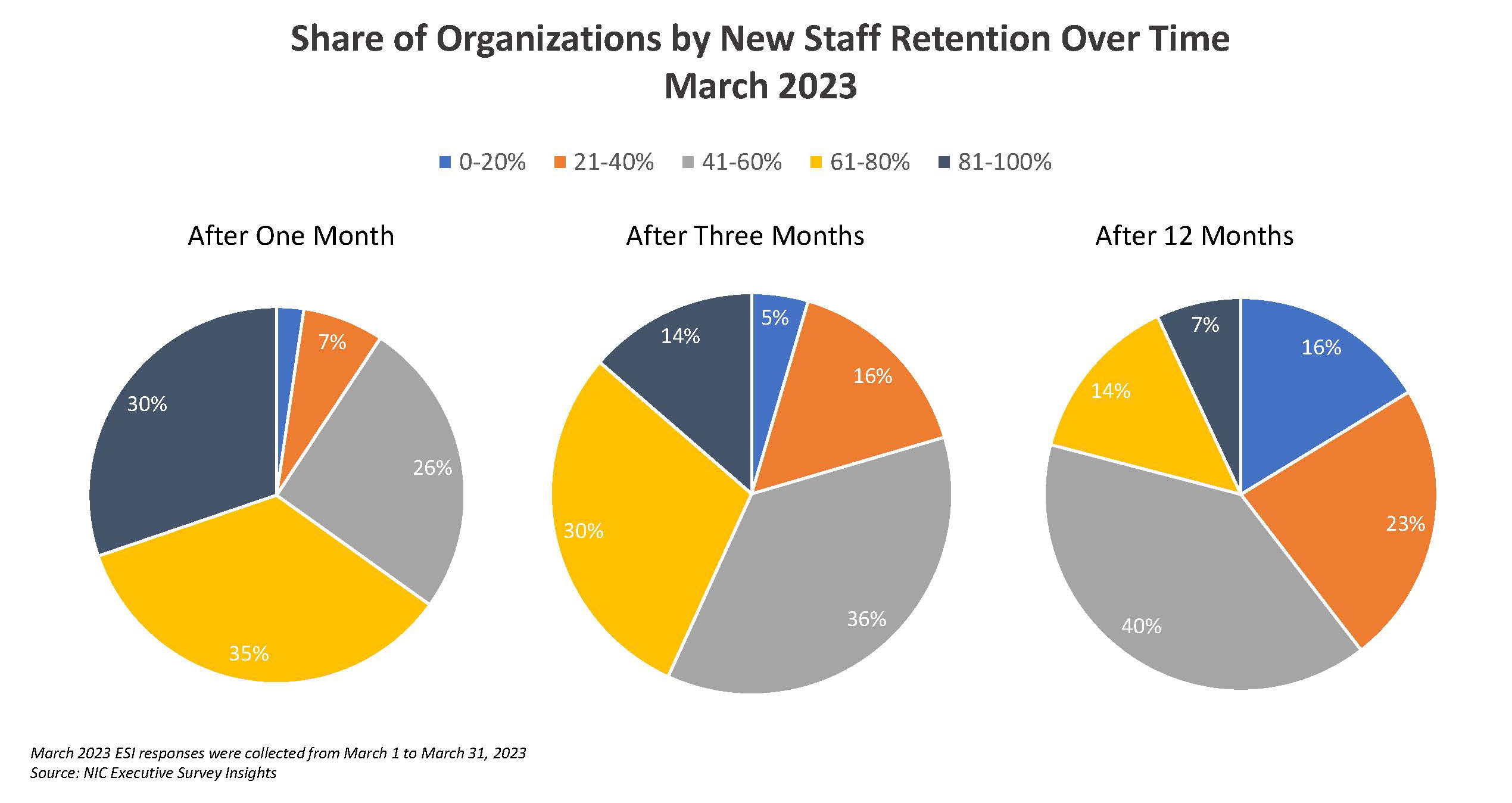
In a recent survey of post-acute and senior housing executives conducted by NIC (National Investment Center) only 30% of organizations noted retention of 80% of their new hires longer than a month. A year ago, this number was 46%. When looking out a year, only 7% of organizations retained more than 80% of their new hires for more than a year. I can only think of one word to describe this data – YIKES!
No magic bullets are available to remedy this issue. Turnover has lots of causes and organizations can only do so much. We have a supply problem in the industry and until the supply is increased, by societal value shifts and proper public policy, turnover will continue to be an issue. I do, however, know organizations that have made an impact and with the implementation of certain strategies, performed better in terms of turnover. These strategies comprise my top five tips/recommendations for improving staff retention.
- IMPROVE MANAGEMENT: This is not easy, but it does immediately and over the longer term, bear real results. Staff don’t work for companies; they work for leaders. Hire leaders that have proven track records in building teams and retaining staff. Don’t promote people without a prior, successful training program in management/supervision. Provide ongoing training in management and supervision.
- RELEASE AS MUCH CONTROL AS POSSIBLE OF THE SCHEDULE: Give staff say in what hours they work, when they work, etc. Of course, parameters are required but if any one major gripe can be alleviated, scheduling is a prime complaint. Staff need to be engaged directly and provided opportunity to address their own work /life balance. Team scheduling is awesome as are incentives around team performance in this regard. Likewise, stop thinking about shifts and how many staff per patient. Look at work blocks and patient needs and when duties really need to be done and by whom.
- RESTRUCTURE REWARD AND COMP: To the extent possible, flex everything and create for new staff, a very stepped process of achieving ongoing rewards/increases in pay and certain benefits like time-off, during that first year. Gainshare as much as possible as well. This is not about pay per se but about recognition and engagement. Everything needs to be on the table. Start with the total comp budget and note, “what’s the best way to spend it” – ROI v. wages and benefits. The more staff feel connected such that what they do correlates to a reward, a benefit or recognition to them (individual and team), the more they are likely to stay.
- ALGEBRA/SIMPLIFY: For decades, I have worked with and led organizations in healthcare that simply can’t stop themselves from doing dumb things. Often, the excuse is “regulation”. My answer: B.S. Rarely is all of the paperwork, forms, redundancy, etc., required or if it is, it can be simplified. Healthcare loves paper, regulations, rules, etc. Staff get trapped here and supervisors use bureaucracy like a hammer – a blunt instrument. My advice, deconstruct. Remove as much needless and redundant chores, paper, etc. from staff. Look acutely at who has to do what by when and then, look at how it is currently being done. Improvement is definitely possible. Pay very close attention to how much additional, non-nursing work nurses and nursing staff are doing.
- INJECT FUN INTO WORK: Healthcare is too serious and too bureaucratic. Give staff a chance to create an environment that encourages team, fun, fellowship. This is within the workplace and outside of work as well. The reality is that staff that feel part of something bigger, committed to each other, enjoy being part of a cause, etc., work harder and stay longer at their place of employment. This requires a culture shift for most healthcare organizations and a definite shift in management style.