
Earlier this year, in January, I wrote a piece on the start of site-neutral payments via a CMS final rule tied to the Outpatient PPS (OPPS). This post is a follow-up of sorts to the January post. January’ post is available here: https://rhislop3.com/site-neutral-payments-kick-0ff/
Hospital ownership has too often become a pricing strategy. A physician office can deliver a routine service, then become a hospital outpatient department after acquisition and command a materially higher Medicare payment for essentially the same care. This guide to Medicare site-neutral payments explains why that arrangement is now squarely in policymakers’ crosshairs and why operators should treat the issue as a strategic planning matter, not another Washington debate.
What Medicare Site-Neutral Payments Actually Mean
Site-neutral payment policy is straightforward in principle: Medicare should pay comparable rates for comparable services regardless of whether they are delivered in a hospital outpatient department, an ambulatory surgery center, or a physician office. The current system does not consistently operate that way.
Medicare generally pays hospital outpatient departments under the Outpatient Prospective Payment System and physician practices under the Physician Fee Schedule. Those payment systems reflect different statutory structures, cost assumptions, and historical compromises. The result is a persistent price differential that can have little to do with the acuity of a particular service or the resources required to furnish it.
The policy case is not that every healthcare setting is interchangeable. A hospital campus carries real standby capacity, emergency readiness, regulatory obligations, specialized infrastructure, and higher-acuity patient mix. The question is narrower and more consequential: when a service can safely be delivered in a lower-cost setting, why should Medicare pay a premium simply because of the billing entity’s ownership structure or address?
That distinction matters. A poorly designed site-neutral policy could underfund hospitals that genuinely provide complex, safety-net, or round-the-clock care. A disciplined policy can instead separate the cost of essential hospital capacity from an avoidable facility-fee advantage on routine outpatient services.
Why the Issue Has Returned to the Center of Medicare Policy
Site neutrality sits at the intersection of three pressures Medicare can no longer ignore: spending growth, consolidation, and beneficiary affordability. Each acquisition of a community physician practice by a health system can shift services into a higher-paid billing category. Medicare spending rises, and beneficiaries may face higher coinsurance tied to the hospital outpatient charge.
This is why site neutrality is not merely a reimbursement debate. It is an anti-consolidation policy, a beneficiary-cost policy, and a Medicare solvency policy. It addresses an incentive that rewards organizational form over efficient care delivery.
MedPAC has repeatedly supported a more rational approach to equalizing payments across settings. Bipartisan policymakers have also advanced versions of site-neutral reform, usually focused on selected ambulatory services that are commonly performed in physician offices. The political appeal is obvious: the policy can generate federal savings without cutting benefits or shifting costs to beneficiaries.
But the details determine whether it is sound reform or blunt budget cutting. Congress has broader authority to redesign payment rules and capture substantial savings. CMS can act within its existing authority, but its room is more limited and its rules remain vulnerable to litigation. The agency’s site-neutral payment approach for clinic visits in certain off-campus hospital outpatient departments demonstrated both the policy direction and the legal friction that accompanies it.
Example: CMS Proposal on Site-Neutral Imaging Payments
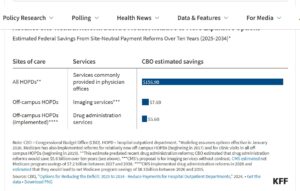
The Centers for Medicare & Medicaid Services (CMS) recently released the 2027 proposed rule for Medicare’s Hospital Outpatient Prospective Payment System (OPPS). Among other provisions, the rule would expand site-neutral payment reforms to certain imaging services furnished in off-campus hospital outpatient departments (HOPDs) .Site-neutral payment reforms aim to align Medicare reimbursement for the same service across different care settings, while preserving appropriate safety and quality safeguards.
Beginning in 2027, CMS proposes to reduce reimbursement by 60 percent for certain imaging services without contrast, such as X-rays and MRIs, when those services are provided in off-campus HOPDs. The goal is to bring payments for these services more closely in line with reimbursement in lower-cost settings.
The proposal would not apply to most rural hospitals. Critical access hospitals are not paid under OPPS, and the proposed change would exclude rural sole community hospitals. Together, these exclusions mean that most rural hospitals—approximately 79 percent—would not be affected.
The Administration’s proposed changes would further advance site-neutral payment reform for certain imaging services. However, as with prior reforms, the proposal remains relatively modest compared with broader options raised by MedPAC and others.
The Financial Exposure Is Uneven
Health systems should resist the temptation to view site neutrality as a uniform percentage reduction. Exposure varies sharply by service line, outpatient footprint, payer mix, location, and the degree to which acquired physician practices have been converted to provider-based billing.
Organizations with large off-campus outpatient networks and significant volumes of routine evaluation and management services, imaging, infusion, and other ambulatory procedures may face the greatest pressure. The financial impact can extend beyond direct Medicare revenue. Commercial payers frequently watch Medicare policy closely, and employers are increasingly unwilling to accept facility-fee escalation for services available in lower-cost settings.
For hospitals, the central risk is not simply less revenue. It is the potential unraveling of an acquisition model that has used outpatient alignment to build referral networks and protect market share. A health system that paid a premium for physician practices based partly on expected hospital outpatient reimbursement may find that its investment thesis has changed.
That does not mean every integrated delivery system is economically suspect. Integration can improve care coordination, clinical governance, specialty access, and population-health management. Yet leaders should be candid about the difference between clinical integration and reimbursement arbitrage. Policymakers increasingly are.
A Guide to Medicare Site-Neutral Payments for Operators
The right management response is not to wait for a final bill or rule. Boards and executive teams should begin with a service-level exposure analysis. Identify which outpatient services are currently paid under hospital outpatient rates, which could be repriced under a physician fee schedule benchmark, and which depend on a higher-acuity hospital environment.
The analysis should distinguish between on-campus and off-campus operations, excepted and non-excepted provider-based departments, and service lines with significant beneficiary cost-sharing implications. A single enterprise-level estimate will conceal the operational decisions that matter most.
Leaders should also pressure-test physician alignment assumptions. If a practice acquisition is under consideration, projected value should not rely on a permanent facility-fee differential for routine care. The more durable acquisition case is built on clinical access, workforce stability, shared data, specialty capacity, and measurable care-management results.
For organizations already operating provider-based clinics, site-neutrality planning should include a hard look at staffing models, scheduling, patient routing, and physical footprint. Some services may remain viable only if delivered with a lower-cost operating model. Others may warrant consolidation into locations where hospital-level resources are clinically necessary and demonstrably used.
What Post-Acute and Senior Living Leaders Should Watch
Site-neutral payment reform is aimed primarily at outpatient payment differentials, but its implications reach well beyond hospital finance. Post-acute operators and senior living executives should view it as another signal that federal policymakers are looking for payment systems that reward appropriate setting, measurable value, and lower total cost of care.
For skilled nursing, home health, hospice, and senior housing organizations, that can create opportunity. If hospitals face greater pressure to manage ambulatory care efficiently, they may become more serious partners in preventing avoidable admissions, accelerating safe transitions, and building clinically credible alternatives to institutional care.
Still, the opportunity should not be romanticized. Hospital systems under revenue pressure may seek to retain more services internally, tighten referral relationships, or demand more favorable partnership economics. Post-acute providers need data that demonstrates their value in terms hospital executives and Medicare policymakers recognize: readmission reduction, lower emergency department utilization, timely discharge, quality performance, and patient outcomes.
Life plan communities and assisted living operators should pay attention as well. The policy logic behind site neutrality reinforces a broader preference for care delivered in the least intensive setting consistent with patient safety. Organizations that can support aging in place, coordinate primary and specialty care, and identify deterioration before it becomes an emergency will be better positioned as payment policy evolves.
The Trade-Off Policymakers Cannot Ignore
The strongest argument against expansive site neutrality is that hospitals are not simply larger physician offices. Many carry losses from emergency care, trauma services, behavioral health, teaching programs, and uncompensated care. Cutting outpatient payments without confronting those obligations could worsen the financial condition of hospitals that communities cannot afford to lose.
That concern is real, especially in rural markets and for safety-net institutions. It is not, however, a sufficient argument for preserving indiscriminate payment differentials. If Medicare intends to subsidize essential community capacity, it should do so transparently through policies targeted to that purpose, not through higher prices for routine services wherever they happen to be billed.
This is the strategic test for the industry: can it defend higher payments with evidence of higher clinical complexity, patient risk, or necessary infrastructure? Where the answer is yes, policymakers should account for it. Where the answer is no, the payment differential is increasingly difficult to justify.
The organizations that will navigate this shift best will not frame site neutrality as an external threat alone. They will use it as a forcing function to clarify which outpatient assets create clinical value, which depend on legacy reimbursement rules, and which care models deserve investment regardless of where Medicare draws the next payment line.