The mandatory Transforming Episode Accountability Model (TEAM) will advance CMS prior work on value-based care models, including bundled care initiatives. The TEAM model (participation) will be mandatory for selected hospitals and participation “optional” for post-acute care providers. Transforming Episode Accountability Model (TEAM) | CMS
The Transforming Episode Accountability Model (TEAM) is set to be a compulsory, episode-based, alternative payment model. Selected acute care hospitals will be tasked with coordinating care for individuals with Traditional Medicare who are undergoing one of the surgical procedures included in the model. These hospitals will initiate an episode and take on the responsibility for the cost and quality of care from the time of surgery until 30 days post-discharge.
The Centers for Medicare & Medicaid Services (CMS) have utilized Core-Based Statistical Areas (CBSAs) to determine the specific geographic regions for the model’s test phase. Hospitals that receive payments under the Inpatient Prospective Payment System (IPPS) and are situated within these CBSAs will be mandated to participate in TEAM. CMS will provide a one-time voluntary opt-in for hospitals that are participating until the last day of the final performance period in the BPCI (Bundled Payments for Care Improvement) Advanced model, or the last day of the final performance year in the CJR (Comprehensive Care for Joint Replacement) model, to join TEAM. For background, I wrote about BPCI and CJR when they were first introduced – https://rhislop3.com/2015/12/01/bundled-payments-final-hip-and-knee-rule/
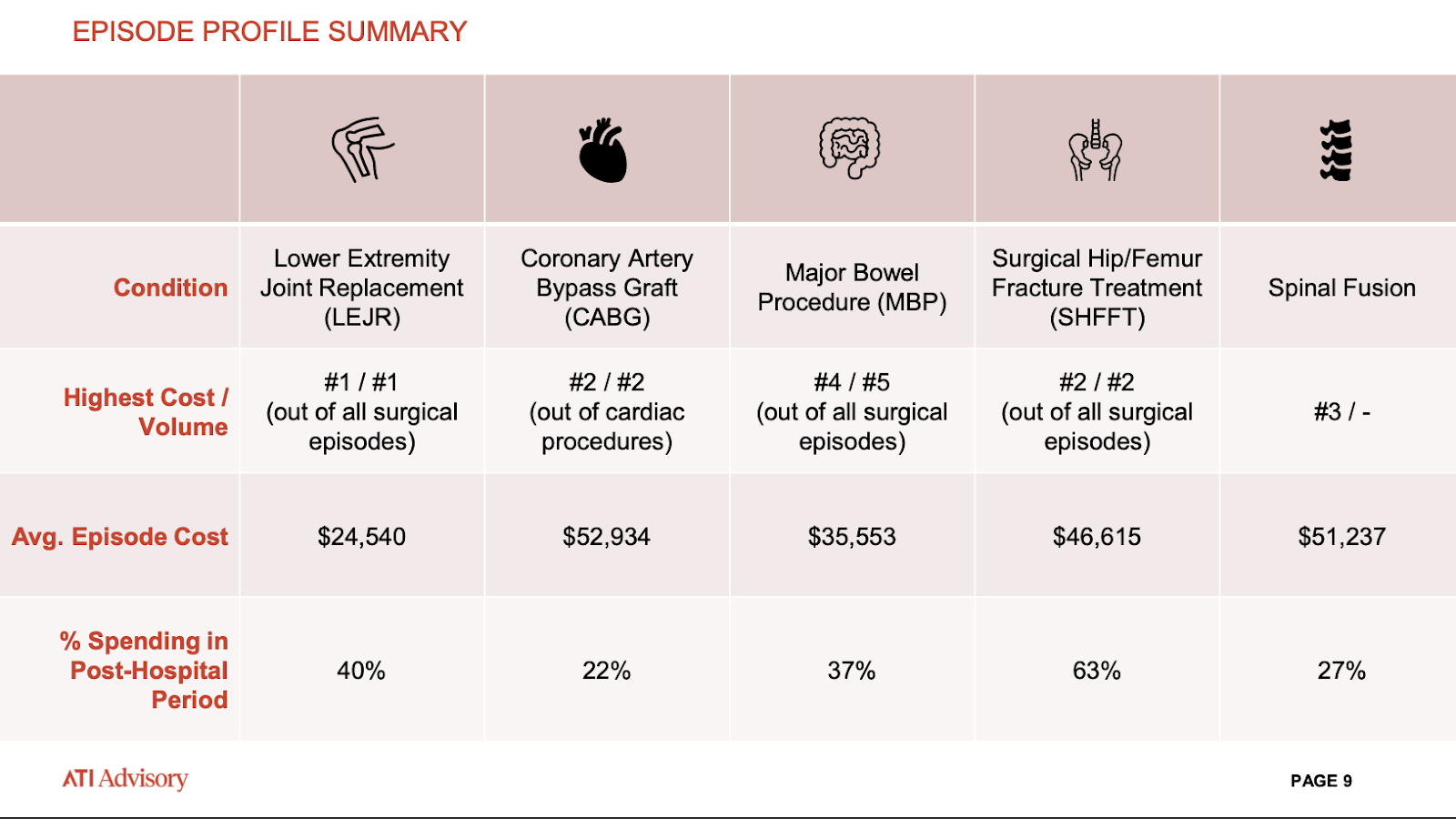
TEAM concentrates on five principal surgical conditions originating in the acute-care hospital setting. These procedures encompass lower extremity joint replacements (primarily hips and knees), coronary artery bypass grafts, significant bowel surgeries, treatments for surgical hip or femur fractures, and spinal fusions. TEAM-FactSheet_8_1_24

CMS is deliberately permitting significant overlap with other bundled payment models, such as existing ACOs or ACO REACH, primarily to test how bundles or episodes of care function in conjunction with each other concerning the total cost of care.
If a beneficiary under TEAM receives a savings payment from CMS, it will not be deducted from the ACO’s funds. Similarly, if there are losses and the TEAM hospital is indebted to CMS, this will not offset any funds allocated to the ACO.
Where opportunities exist, though not specific for post-acute providers, is in the realm of care coordination and post-hospitalization care. CMS does not specifically address post-acute providers in the TEAM program. The role for SNFs for example, is that of collaborator, if chosen by the participating hospital to fulfill a post-discharge care role. The same will be true for home health agencies.
Post-acute providers that are comfortable managing episodes of care can position themselves as segment (post-discharge) partners and become value-based care participants with hospitals. TEAM could be an exceptional opportunity for post-acute providers that have BPIC or CJR experience or have developed post-discharge partnerships with hospitals.
The agreement under TEAM is between CMS and the hospital. The hospital could select post-acute providers as “collaborators,” to manage whatever percentage of care is needed post-hospital discharge. Creatively, this offers massive opportunities for SNFs to partner with home health agencies and even with Assisted Living Facilities that can provide integrated post-hospital care.
TEAM is planned to launch in January 2026. The common payment methodology is episodes of care, based on a target price that imputes a 3% discount. The model will run for five years. The hospital must perform 3% better for the overall episode of care, and then CMS essentially takes 3% off the top.
Any dollar after the 3% that gets created goes/gets paid to the participants. For example, if a hospital generates $5,000 on its qualifying episodes above that 3% target, all $5,000 can be used for payback, shared with participants, used for quality improvement, etc. Hospitals act as the bundler and hold complete accountability for spending within this model. The graphic below is courtesy of the consulting firm ATI.